Eviva, formerly Puget Sound Surgical Center, is the most published bariatric ASC facility. Our research spans surgical techniques, body composition, and long-term outcomes, reflecting our commitment to advancing bariatric care.
Introduction
Predictors of long-term weight loss in sleeve gastrectomy(SG) currently do not exist. We reviewed our long term data in a single private practice to assess for variables that will help surgeons predict weight loss failure early after SG.
Objective
To create weight prediction models to aid in the evaluation of the adequacy of short-term weight loss post SG on long-term weight maintenance.
Methods
491 patients undergoing SG in a Private Practice setting were included in the study. Data was collected retrospectively from March 2011 through September 2013. Percent excess weight loss (EWL) was calculated for each patient at 3 months and 1 year. Linear regression was performed on all patients with greater than 1 year follow up in order to interpolate their weight at 1 year. Patients were included only if they had at least 3 follow up visits and their weight loss could be modeled with a R2
Results
Patients were divided into EWL quartiles. The patients quartiles were as follows at three months quartile 1 7-33%, quartile 2 34-41%, quartile 3 42-51%, quartile 4 >51%. Patient’s weight loss tended to remain in the quartile they were in at their 3 month visit, especially those in the 1st and 4th quartiles. The positive and negative predictor values at 12 months for the 1st quartile results were 70% and 84% respectively.
Conclusions
We are the first group with data documenting that short-term weight loss can predict long-term weight loss success or failure quite accurately. Identifying failure early is critical to the long-term success of the bariatric patient. This knowledge will allow surgeons to discuss intervention such as medication, lifestyle or conversion to gastric bypass or duodenal switch reoperations at three months rather than waiting years for weight regain to occur.
Abstract
Background: Sleeve gastrectomy (SG) is currently the most widely performed procedure for the treatment of obesity. SG leads to significant weight loss as well as a reduction in weight-related comorbidities. Rapid weight loss after bariatric surgery (BS) produces changes in body composition; however, these changes are not well documented in the early stages post-SG, when the greatest weight change occurs.
Objective: To identify changes in body composition in the early stages following SG.
Setting: Eviva Bariatrics, Seattle, WA.
Methods: Demographics were collected for all patients who underwent SG at Eviva Bariatrics and also underwent pre- and postoperative biometric testing. Changes in fat-free mass (FFM), fat mass (FM), and body fat percentage (BF%) were measured using the BodPod. Testing occurred on average 74 days postoperatively (range 37–136 days). Testing protocols followed BodPod guidelines, and all measurements were performed on the same machine to ensure accuracy.
Results: Sixty-one SG patients from January 2014 to April 2016 underwent biometric testing. On average, patients lost 39.9% of excess body weight (EWL) and 15.2% of total body weight by 74 days post-op. Average BF% dropped from 49.4% to 45.0%. Patients lost an average of 27% of their FFM by 74 days. Three patients (4.9%) maintained or increased FFM post-op, while six patients (9.8%) lost more FFM than FM, leading to an increase in BF%.
Conclusion: The goal of BS is to reduce weight and weight-related comorbidities. However, weight reduction alone is not sufficient to assess success post-SG. Patients losing more FFM than FM should be identified early to optimize outcomes. Achieving a healthy body composition, rather than only focusing on weight loss, should be emphasized. Future studies should identify factors influencing FFM preservation and evaluate long-term body composition results in SG patients.
Background
Currently there are no models to predict a patient’s ability to succeed at a surgery before they receive it. Because of this many surgeons disagree on what procedures to offer to their patients and what variable should influence this decision.
Objective
To create a statistical model that predicts failure in a sleeve patient before surgery.
Methods
491 patients undergoing SG in a Private Practice setting were included in this study. Data was collected retrospectively from March 2011 through September 2013. Percent excess weight loss (EWL) was calculated for each patient at 1 year. Linear regression was performed on all patients with greater than 1 year follow up in order to interpolate their weight at 1 year. Patients were included only if they had at least 3 follow up visits and their weight loss could be modeled with a R2>0.95.
Results
Patients were divided into EWL quartiles. The patients quartiles were as follows at one year quartile 1 9-54%, quartile 2 55-68%, quartile 3 69-84%, quartile 4 >85%. Patients in the first quartile at one year were defined as failing the procedure. The positive and negative predictor values for our model were 58% and 81% respectively with sensitivity at 33% and specificity at 92%. The multivariate analysis indicated that diabetes, sleep apnea, and preoperative BMI were statistically significant
Conclusions
We are the first group to show that weight loss at 1 year can be predicted before the surgery is performed. Patients with sleep apnea, diabetes, and a BMI greater than 48 should not be offered a sleeve gastrectomy because of the high failure probability

Context
The mechanisms mediating the short- and long-term improvements in glucose homeostasis following bariatric/metabolic surgery remain incompletely understood.
Objective
To investigate whether a reduction in adipose tissue inflammation plays a role in the metabolic improvements seen after bariatric/metabolic surgery, both in the short-term and longer-term.
Design
Fasting blood and subcutaneous abdominal adipose tissue were obtained before (n=14), at one month (n=9), and 6–12 months (n=14) after bariatric/metabolic surgery from individuals with obesity who were not on insulin or anti-diabetes medication. Adipose tissue inflammation was assessed by a combination of whole-tissue gene expression and flow cytometry-based quantification of tissue leukocytes.
Results
One month after surgery, body weight was reduced by 13.5±4.4 kg (p<0.001), with improvements in glucose tolerance reflected by a decrease in area-under-the-curve (AUC) glucose in 3-h oral glucose tolerance tests (−105±98 mmol/L*min; p=0.009) and enhanced pancreatic β-cell function (insulinogenic index: +0.8±0.9 pmol/mmol; p=0.032), but no change in estimated insulin sensitivity (Matsuda insulin sensitivity index [ISI]; p=0.720). Furthermore, although biomarkers of systemic inflammation and pro-inflammatory gene expression in adipose tissue remained unchanged, the number of neutrophils increased in adipose tissue 15–20 fold (p<0.001), with less substantial increases in other leukocyte populations. By the 6–12 month follow-up visit, body weight was reduced by 34.8±10.8 kg (p<0.001) relative to baseline, and glucose tolerance was further improved (AUC glucose −276±229; p<0.001) along with estimated insulin sensitivity (Matsuda ISI: +4.6±3.2; p<0.001). In addition, improvements in systemic inflammation were reflected by reductions in circulating C-reactive protein (CRP; −2.0±5.3 mg/dL; p=0.002), and increased serum adiponectin (+1,358±1,406 pg/mL; p=0.003). However, leukocyte infiltration of adipose tissue remained elevated relative to baseline, with pro-inflammatory cytokine mRNA expression unchanged, while adiponectin mRNA expression trended downward (p=0.069).
Conclusion
Both the short- and longer-term metabolic improvements following bariatric/metabolic surgery occur without significant reductions in measures of adipose tissue inflammation, as assessed by measuring the expression of genes encoding key mediators of inflammation and by flow cytometric immunophenotyping and quantification of adipose tissue leukocytes.
Keywords: adipose tissue inflammation, bariatric surgery, metabolic surgery, insulin resistance
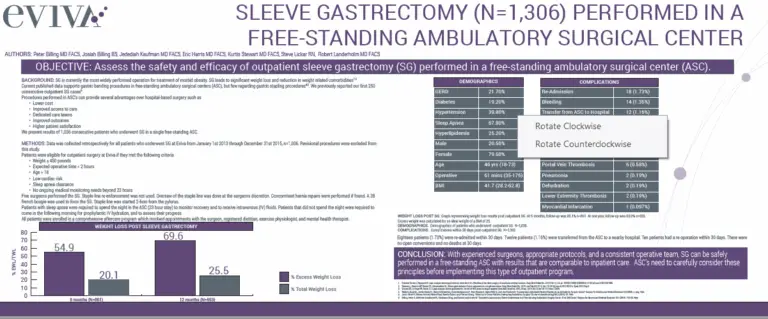
Sleeve gastrectomy (SG) is currently the most widely performed procedure for the treatment of morbid obesity. SG leads to significant weight loss as well as a reduction in weight related comorbidities. Procedures performed in ambulatory surgical centers (ASC) can provide several advantages over hospital-based surgery. We present our results of 1036 consecutive patients who underwent SG in an ASC.

Background
Procedures performed in ambulatory surgical centers (ASC) can provide several advantages over hospital-based surgery. Understandably, concerns have been raised regarding “high acuity” cases in the ASC setting. Recently the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) presented protocols for ASCs to follow, requiring them to perform only “low acuity” cases to be compliant with accreditation.
Sleeve gastrectomy (SG) is currently the most widely performed operation for treatment of morbid obesity. There are many patients that fall outside NIH criteria that suffer with obesity and the associated comorbidities of their condition. SG leads to significant weight loss and reduction in weight related comorbidities. We know low BMI patients can benefit from WLS as well and our aim is to study the outcomes of low BMI patients in our surgery center. Procedures performed in ambulatory surgical centers (ASC) can provide several advantages over hospital-based surgery. We present results of 181 patients with a body mass index (BMI) < 35 who underwent SG in a free-standing ASC.
Laparoscopic sleeve gastrectomy (SG) is now the most widely performed bariatric surgery. The impact of SG on gastroesophageal reflux disease (GERD) remains a topic of debate amongst bariatric surgeons. Furthermore, some payers will not cover SG in the presence of pre-operative GERD.

Abstract
Background: A growing body of evidence supports the laparoscopic sleeve gastrectomy (LSG) as a safe and effective procedure for sustained weight loss and amelioration of weight-related co-morbidities. Procedures performed in ambulatory surgery centers (ASC) can provide several advantages over hospital-based surgery. We present our results of 250 consecutive patients undergoing LSG in an ASC. The objective of this study was to assess the safety and efficacy of outpatient LSG in a freestanding ASC.

Background: Sleeve gastrectomy (SG) is currently the most widely performed operation for treatment of morbid obesity. SG leads to significant weight loss and reduction in weight related comorbidities. Procedures performed in ambulatory surgical centers (ASC) can provide several advantages over hospital-based surgery. We present results of 2,528 consecutive patients who underwent SG in an ASC.
Laparoscopic adjustable gastric band (LAGB) was a common weight loss surgery for many years, but often results in poor long-term weight loss and complications. Removal of gastric band and conversion to sleeve gastrectomy (SG) is safe as either a 1-step or 2-step operation. We present a 2-step removal of LAGB and conversion to SG that was complicated by a proximal gastric obstruction. The proximal gastric obstruction was not relieved with stenting or balloon dilation, so an operation was performed, revealing an interesting mechanism of obstruction and unforeseen solution.
Background: Endoscopic sleeve gastroplasty (ESG) is a less invasive alternative to laparoscopic sleeve gastrectomy (LSG) for bariatric intervention in patients. Recent propensity matched analyses have demonstrated non-inferior weight loss for ESG compared to LSG analyses, with comparable adverse event rates. However, there is a lack of comparative costing data to inform clinical and economic decision making.
Aim: To compare short-term costs between ESG and LSG in US patients undergoing bariatric intervention.
Material & Methods: A cost-consequence model was developed to simulate procedural and adverse event cost up to 30 days. Clinical and cost parameters were informed using commercial US claims databases, targeted literature review and expert opinion.
Results: A significantly greater amount of ESG procedures took place in the outpatient setting (p<0.01). ESG was associated with a reduction in costs ($4,452 per patient) at 30 days, compared to LSG. Savings were driven by a reduced OR time ($871) and Length of stay ($2,776) between the procedures. After 30 days there was an increased incidence of gastroesophageal reflux disease (6.6%) in the LSG compared to ESG (0.4) (p<0.01). All other adverse events contributed to a cost saving with ESG after 30 days.
Conclusion: In our analysis, ESG is cost-saving compared to LSG and may offer economic benefits for selected US bariatric patients. Cost-saving were due to procedure setting and reduction in facility resource utilisation at 30 days. Well conducted and longer-term costing studies are required to inform robust economic modelling and clinical decision making.
Abstract
Introduction: Endoscopic sleeve gastroplasty (ESG) has gained popularity over the past decade and has been adopted in both academic and private institutions globally. We present outcomes of the largest cohort of patients from the United States undergoing ESG and evaluate these according to obesity class.
Methods: We performed a retrospective analysis of adult patients who underwent ESG. Medical information was abstracted from the electronic record with weight records up to 2 years after ESG. Percent total body weight loss (%TBWL) at 6, 12, 18, and 24 months was calculated based on baseline weight at the procedure. SPSS (version 29.0) was used for all statistical analyses.
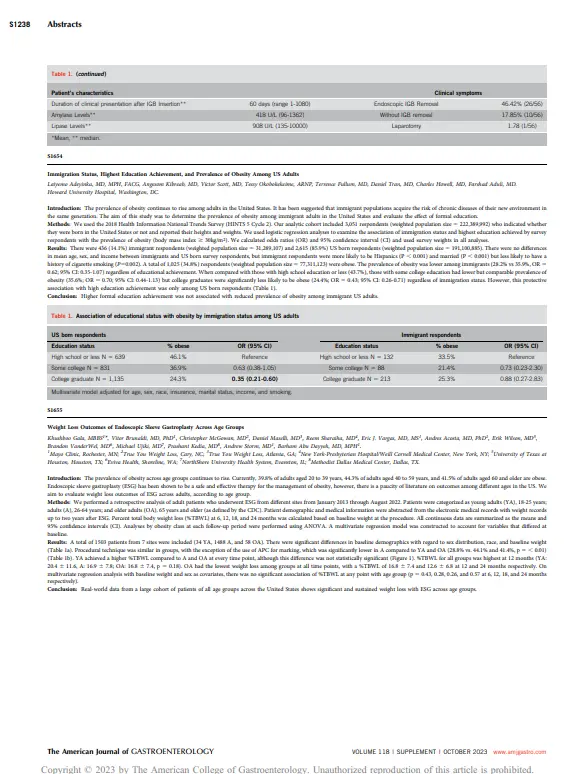
Results: A total of 1,506 patients from 7 sites were included (501 Class I obesity, 546 Class II, and 459 Class III). Baseline demographics differed according to obesity class due to differences in age, body mass index (BMI), height, sex distribution, and race. As early as 6 months post-ESG, mean BMI for each class dropped to the next lower class and remained there through 2 years. %TWBL achieved in the Class III group was significantly greater when compared with other classes at all time points. At 12 months, 83.2% and 60.9% of patients had ≥10% and ≥15% TBWL for all classes. There were no differences in adverse events between classes.
Discussion: Real-world data from a large cohort of patients of all BMI classes across the United States shows significant and sustained weight loss with ESG. ESG is safe to perform in a higher obesity class with acceptable midterm efficacy.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Abstract
Introduction: Endoscopic sleeve gastroplasty (ESG) is performed in clinical practice by both gastroenterologists and bariatric surgeons across the nation. Given the increasing regulatory approval and global adoption, our aim is to evaluate real world outcomes in multidisciplinary practices involving bariatric surgeons and gastroenterologists (GI) across the United States. Methods: We included adult patients with obesity who underwent ESG from January 2013 to August 2022 in clinical US practices. Patients and procedural characteristics, serious adverse events (SAEs), and weight loss outcomes up to 24 months were analyzed. SPSS (version 29.0) was used for all statistical analyses. Results: 1506 patients from 7 sites included 235 (15.6%) treated by surgeons and 1271 (84.4%) treated by GIs. There were no significant baseline differences between groups (Table 1). GIs used Argon Plasma Coagulation (APC) for marking more often than surgeons (34.8% vs. 3.4% p-value < 0.001). There were no differences between providers in overtube use, or intraprocedural complications. The mean number of sutures was 7 and was similar between the two groups. On average, procedural length was 20 minutes longer for surgeons compare to GIs (p0.05). Conclusion: Clinical data from a large US cohort showed significant and sustained weight loss with ESG and excellent safety profile in both bariatric surgery and GI practices. This supports the scalability of the procedure across practices in a multidisciplinary setting.
Introduction:
The prevalence of obesity across age groups continues to rise. Currently, 39.8% of adults aged 20 to 39 years, 44.3% of adults aged 40 to 59 years, and 41.5% of adults aged 60 and older are obese. Endoscopic sleeve gastroplasty (ESG) has been shown to be a safe and effective therapy for the management of obesity, however, there is a paucity of literature on outcomes among different ages in the US. We aim to evaluate weight loss outcomes of ESG across adults, according to age group.
Abstract
Background and Aims
Endoscopic sleeve gastroplasty (ESG) is an effective, minimally invasive gastric remodeling procedure to treat mild and moderate obesity. Early adoption of ESG may be desirable to try to halt progression of obesity, but there are few data on its efficacy and safety for overweight patients.
Methods
This was a multicenter, international, analytical case series. Six U.S., 1 Brazilian, 1 Mexican, and 1 Indian center were included. Overweight patients according to local practice undergoing ESG were considered eligible for the study. The end points were percent total weight loss (%TWL), body mass index (BMI) reduction, rate of BMI normalization, and rate of adverse events.
Results
One hundred eighty-nine patients with a mean age of 42.6 ± 14.1 years and a mean BMI of 27.79 ± 1.17 kg/m2 were included. All procedures were successfully accomplished, and there were 3 intraprocedural adverse events (1.5%). The mean %TWL was 12.28% ± 3.21%, 15.03% ± 5.30%, 15.27% ± 5.28%, and 14.91% ± 5.62% at 6, 12, 24, and 36 months, respectively. At 12 and 24 months, 76% and 86% of patients achieved normal BMI, with a mean BMI reduction of 4.13 ± 1.46 kg/m2 and 4.25 ± 1.58 kg/m2. There was no difference in mean %TWL in the first quartile versus the fourth quartile of BMI in any of the time points. However, the BMI normalization rate was statistically higher in the first group at 6 and 12 months (6 months, 100% vs 48.5% [P < .01]; 12 months, 86.2% vs 50% [P < .01]; 24 months, 84.6% vs 76.1% [P = .47]; 36 months, 86.3% vs 66.6% [P = .26]).
Conclusions
ESG is safe and effective in treating overweight patients with high BMI normalization rates. It could help halt or delay the progression to obesity.
Abbreviations
%TWL (percent total weight loss)
AE (adverse event)
BMI (body mass index)
ESG (endoscopic sleeve gastroplasty)

Abstract
Background
To evaluate the weight loss outcomes of the large US cohort of patients undergoing endoscopic sleeve gastroplasty (ESG) with or without concomitant anti-obesity (AOM) use.
Methods
We performed a retrospective analysis of adult patients who underwent ESG from seven different sites, from January 1, 2020 to November 30, 2022. Percent total body weight loss (%TBWL) and %excess weight loss (%EWL) were calculated based on baseline weight at the procedure. Medication use was considered if the subject received a prescribed AOM during the study period. SPSS (version 29.0) was used for statistical analyses.
Results
A total of 1506 patients were included (1359 (90.2 %) no AOM use and 147 (9.8 %) AOM use). Patients who were on an active AOM at the time of the procedure had a significantly lower TBWL% as compared to patients not on AOMs at 6 months. At the 24-month visit, patients who were prescribed AOMs after the 12-month visit had a significantly higher TBWL% and EWL% as compared to patients who were on active AOM at the time of the procedure. There was no significant difference between classes of medications at any time point, however, patients on a GLP-1RA had a trend towards improved weight loss at 18 and 24 months.
Conclusion
In this large, real-world cohort of patients from the United States, data signal that with the use of pharmacotherapy at the appropriate time, patients can achieve optimal results.
Abstract
Obesity affects over 650 million adults globally, yet laparoscopic bariatric surgery, despite 60%-80% excess weight loss and <1% adoption, remains underutilized. Endobariatric therapies, including endoscopic sleeve gastroplasty (ESG), intragastric balloons, and transoral outlet reduction (TORe), expand treatment options, offering minimally invasive alternatives for patients averse to surgery’s risks or permanence. ESG achieves 15% to 20% total body weight loss (TBWL), TORe 8% to 12%, with adverse events below 2%. These tools salvage high-risk cases, revise weight regain, and manage complications, synergizing with GLP-1 agonists for enhanced outcomes (e.g. ESG plus GLP-1: 20.5% TBWL). Integration demands endoscopic expertise, amplifying bariatric practice reach and efficacy.

Abstract
Background and study aims Endoscopic sleeve gastroplasty (ESG) is performed in clinical practice by gastroenterologists and bariatric surgeons. Given the increasing regulatory approval and global adoption, we aimed to evaluate real-world outcomes in multidisciplinary practices involving bariatric surgeons and gastroenterologists across the United States.
Patients and methods We included adult patients with obesity who underwent ESG from January 2013 to August 2022 in seven academic and private centers in the United States. Patient and procedure characteristics, serious adverse events (SAEs), and weight loss outcomes up to 24 months were analyzed. SPSS (version 29.0) was used for all statistical analyses.
Results A total of 1506 patients from seven sites included 235 (15.6%) treated by surgeons and 1271 (84.4%) treated by gastroenterologists. There were no baseline differences between groups. Gastroenterologists used argon plasma coagulation for marking significantly more often than surgeons ( P <0.001). Surgeons placed sutures in the fundus in all instances whereas gastroenterologist placed them in the fundus in less than 1% of the cases ( P ). Procedure times were significantly different between groups, with surgeons requiring approximately 20 minutes more during the procedure than gastroenterologists ( P 10 and >15% TBWL were similar between the two groups at 12, 18, and 24 months. Rates of SAEs were low and similar at 1.7% for surgeons and 2.7% for gastroenterologists ( P >0.05).
Conclusions Data from a large US cohort show significant and sustained weight loss with ESG and an excellent safety profile in both bariatric surgery and gastroenterology practices, supporting the scalability of the procedure across practices in a multidisciplinary setting.
Keywords: GI surgery, Endoscopy Upper GI Tract, Quality and logistical aspects, Performance and complications